I am Amanda, an experienced RN in the state of TN and a PhD candidate exploring the emotional wellbeing of family caregivers.
I would love this to become the site you turn to for health Advocacy, Research, and Education.
Healthcare is a team effort. No one should ever feel alone in the journey to better health. You are a key part of the healthcare team. As a clinician, I recognize that I am a guide through the complexities of healthcare knowledge, processes, and systems. I look forward to using this blog and my services to help you answer your healthcare questions. I hope I can use my experience as an advocate, researcher, and educator to better serve your needs.
I am considering having guest bloggers share their unique stories also.
Healthcare professionals, I hope you find the information on this site to be informative and inspirational. I plan to share with you my experience as a nurse, graduate student, and beyond professionally. I am also planning services geared toward clinicians and academics.
Feel free to email me at armmedical@outlook.com with your healthcare questions, blog post ideas, and how I can serve you. Check out the Services page coming soon.
Together we ARE the team that can make a difference in improving not just health but healthcare.
No information shared should be considered personal healthcare advice. Consult your provider for an individualized plan.
Marjan’s Fasting Firepower has valid points and facts but is definitely a personal opinion piece. Marjan does not usually use primary research to back up his points on the benefits of fasting, but the news media’s interpretation of the research often leads to sensationalization of the results. Scriptural quotes were sometimes taken out of context, and the fasting experts quoted have been marginalized by the science world, not just medical/health scientists. This book was independently published. Thus, has significant formatting issues (at least in the OBC Reader).
Marjan is right that fasting, not only related to nutrition, can significantly impact a person’s emotional, physical, and spiritual health. As a registered nurse, I believe all healthcare clinicians need more training on using food as medicine. I am concerned about how Marjan seems to dismiss the knowledge of registered dieticians and others formally trained in nutrition for individuals with limited scientific training to critique research adequately. At this point, I am quite skeptical of how fasting and eating organic and unprocessed foods can treat or prevent mental illness. Before I can support such claims by Marjan, I will need to see more definitive research.
Not all individuals can follow a fasting routine like Marjan. Those who are impoverished in the inner-city cannot escape air pollution, have limited land to raise their own food, and often can only afford the highly processed and preserved food in the grocery store. Middle-class individuals in suburbia may not have the time or even enough land to raise their own food and often do not make enough money to buy organic foods. Marjan warns individuals with health concerns to work with knowledgeable healthcare clinicians before starting a fasting routine. I embrace this, yet finding such a clinician can be difficulty for most individuals.
I read this book as a free download on the Online Book Club (OBC) Reader application. This application was quite new when I downloaded it, so between the learning curve, the format of quotes within this book, and possible technical glitches, I found this book hard to navigate. It was hard to highlight specific words, especially near quotes and at the beginning of each chapter. If I wanted to make a note and then change the color of the highlighting, I found this impossible. I only found out when reading another book how to delete bookmarks.
Marjan’s Fasting Firepower is a personal, political, and editorial work. The information in it needs to be critically reviewed and communicated by the scientific community, not the testimonial that this book really is. I am actually more interested in Marjan’s other book 600 Devils: From Refugee to Redemption, a life impacted by smuggling, cannabis, psychedelics, conmen, cops, and assorted holy men. This is an area where Marjan is actually an expert; he is only an individual with experience in fasting.
I found it difficult to tell if Tony Selimi’s book The Unfakeable Code fits in a bookstore or library’s nonfiction, self-help, or marketing section. The book starts out with over 15 pages of praise for the book and Tony’s coaching work. The meat of the book, from the Introduction to the second-to-last page about the fifth principle, is only 156 pages. More than 30 additional pages follow. In other words, about 20% of the book markets Selimi’s books and coaching services.
Selimi uses his formal computer programming education to initially explain that a person can rewrite the code for their brain, or how they think about their life, yet limits how much he uses this analogy when discussing the five principles a person should use to change their perspective on one or more areas of their life. The five principles reflect sound psychological principles, and words like masks, facades, and personas are more commonly used than computer terminology.
The Unfakeable Code provides sound psychological advice in the areas of cognitive behavioral therapy and emotion regulation. No one disputes that thinking more objectively or positively about a situation will often lead to more positive actions being taken, yet Selimi is not a psychologist, therapist, or neurologist. Thankfully, he does mention that it is okay to use such professionals, yet includes coaches who, at least in the United States, don’t require formal training or certification to demonstrate competence. Selimi is certified in coaching, but how does that compare to individuals with at least master’s degrees and government-issued licenses in these other professions?
As a registered nurse who has worked in neurology and studied psychology, I really enjoyed this book, found the principles practical, and the activities thought-provoking. Yet, I don’t think Selimi was the best person to write this book. Yes, he has anecdotal evidence that these five principles work. He talks about the science and psychological theories that support these principles but barely touches on how their work aligns with the five principles he discusses.
Finally, I cannot give this book the five out of five stars it deserves, as novum publishing bills itself as being a publisher for first-time authors yet lacks the extra support a first-time author would need. I often had to reread sentences to understand what the author was trying to communicate and found “façade” to be a distracting way of spelling facade. The Unfakeable Code is Selimi’s 2nd full book, along with writing a section in Fit-For-Purpose Leadership #3. I guess popular publishing companies saw The Unfakeable Code as a marketing piece, not a nonfiction or self-help book.
First Survivor is a labor of love and advocacy by author Mark Unger, educating the public not only on being advocates for their loved ones but also seeking out and participating in clinical trials. Unger’s writing pulled at my heartstrings as I rode the roller coaster of emotions of each member of the family, from the bravery of Louis, the anxiety of parents, and the mixed emotions of Harry. I really appreciate that he also incorporated how patient and kind the physicians and nurses were in answering questions and suggesting ways to keep Louis comfortable.
Having been a nurse of adults with cancer at a major teaching a research hospital, I got to see and feel these feelings with families. Unger does a great job blending the family member’s memories and journal entries from in the heat of the cancer battle to help readers also feel the complex emotions and absorb the overwhelming amount of information, in what can seem like a foreign language. Clinicians can forget to adequately explain these terms to overwhelmed families, but through Unger’s questions and seeking answers, he was not able to only better understand the care his son was receiving but also has now educated other families that it is okay to ask questions and seek more information.
I cannot tell if First Survivor is a self-published book or not, but the use of a medical editor may have caught the minor errors as a registered nurse with oncology experience identified in the book. (I read this via the Kindle application.) Minor errors such as the occasionally misspelled medication and some alignment issues in areas such as the table of contents and changing the size of the table on the history of survival between the two pages it is on occurred but did not take away from the strength of the story. I am grateful that Unger decided to include a glossary to help those in the general public learn some of the medical jargon used in cancer care. Yet, I found the additional section called Medical Background redundant, even though it did include some terms not included in the glossary and did go into much further detail for those who might be interested.
As a nurse who has worked with adult cancer clients and is now transitioning into the role of nurse scientist, I really appreciate the effort that was put into First Survivor. I am giving this book 4 out of 5 stars, related to the minor errors above, recognizing Unger’s privilege of being in a high position within the family company allowed him time and financial means to research and advocate for his son’s health and write this book. This is a privilege few have, and I am grateful he used that privilege to break down barriers in healthcare to allow for more family and clinician collaboration and communication. I know many patients of various ages and disease processes are living better lives because of including the patient and family as part of the healthcare team.
This video explains the similarities and differences between stroke and heart attack diagnosis and treatment. It was recorded on 12/22/21 for Chosen Medical Staffing of Nashville, TN.
German neurologists Hans Gerhard Creutzfeldt and Alfons Maria Jakob discovered CJD in the 1920’s.
Disease
Image by CJD Foundation
CJD is a group of fast acting, fatal (usually less than 1 year) neurological diseases caused by prions (normal proteins within the body). These prions change (mutate) to cause CJD.
Multiple forms of CJD exists and no cure exists. Sporadic CJD (sCJD) tends to effect individuals over the age of 60 with no known cause for the infection.
Genetic CJD (gCJD) has a dominant pattern where if one parent has the disease each child would have a 50% chance of inheriting the gene. Multiple genetic mutations are known to increase individuals’ risk for gCJD. Individuals with this form of the disease tend to be younger, 40-60 years old, at the age of onset.
Acquired forms of CJD cause < 1% of US cases. Iatrogenic CJD (iCJD) are associated with medical treatments. Variant CJD (vCJD) come from beef infected with the “mad cow” prion disease, bovine spongiform encephalopathy (BSE or mad cow disease). Individuals with this form of the disease are the youngest to become infected.
Approximately 1 person per million people may be affected by CJD. Approximately 320 new cases are diagnosed in the United States. Most cases (85%) occurring for no know reason. A majority (10-15%) of the remaining cases appear to genetic causes. Rarely, about 1%, CJD cases are related to individuals eating beef with bovine spongiform encephalopathy (BSE or mad cow disease) or via medical procedures.
Causes
See above.
Diagnosis
Examination by a doctor, often a neurologist, and possibly a psychologist or psychiatrist. Neurologists specialize in disorders of the nerves and brain. Psychologists and psychiatrists evaluate individuals’ mental health. (Psychiatrists are medical doctors who can prescribe medications. Psychologists cannot prescribe medications but are more likely to provide individual or group counseling.
Image by chss.org.uk
Blood tests-A needle is poked into a person’s vein and blood is collect in tubes to be tested in a lab. Such tests can rule out other causes, like infection. Genetic testing is also done this way.
Lumbar puncture-A needle is poked into a person’s back to draw out some of the fluid that surrounds the brain and spinal cord. This fluid is called cerebral spinal fluid (CSF). Doctors will send the fluid they collect to the lab to find out if there is another cause for the symptoms, like infection, or if there are abnormal proteins indicative of CJD in the CSF.
Electroencephalogram (EEG)-Small stickers are placed on the client’s head and allow doctors to watch brain wave patterns looking for specific changes noted with CJD. This test may also be used to rule out seizure-like behavior of some clients.
Image by Science ABC
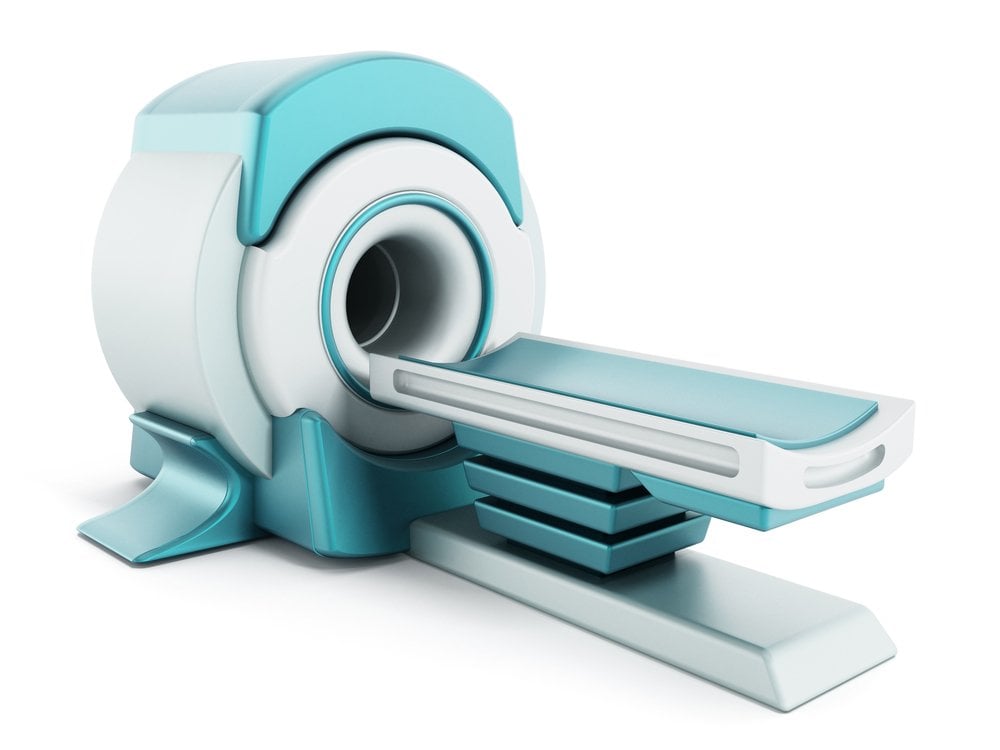
Magnetic Resonance Imaging (MRI)-The client is placed into a scanner like the one pictured on the left. This device uses a magnet to takes pictures so that the doctor can see through the skull to see the brain.
Computed Tomography (CT)-Similar to an MRI, the CT scanner lets doctors and other healthcare providers look at the brain. The machine can take multiple X-rays in a short period of time and creates multiple pictures, slices, of the brain to see the brain structure in more detail than an MRI.
Signs & Symptoms
Brain-Dementia, anxiety and or depression can be seen in in persons with CJD as their brain deteriorates. Family may also note that the person’s personality changes. With certain types of CJD plaques are seen on MRI or CT scans. These plaques are a buildup of materials in the brain that do not let the electrical signals flow through the brain correctly. Difficult sleeping (insomnia) may also occur.
Image by theinterpretersfriend.org.
Eyes-Individuals with CJD may initial present at the eye doctor complaining of blurry vision or vision loss from one side of their eyes (hemianopia).
Muscles-Jerky, repeated muscle movements may be called myoclonus or extrapyramidal side effects (EPS) by your doctor. Difficulty with balance (ataxia) could lead to frequent falls and injuries from the falls.
Mouth-Individuals with CKD may have difficulty speaking or may even quit speaking all together as the facial muscles have less ability to move. This also affects these individuals’ ability to eat.
Treatment
Treatment is considered supportive as there is no cure for CJD. A variety of psychiatric medications may be used to control symptoms of anxiety, depression, personality changes, and at times even muscle jerks. Some individuals with CJD or their family members may choose to have a feeding tube placed to reduce the risk of choking or pneumonia for individuals who have difficulty swallowing.
Individuals with CJD or their families may choose to participate in hospice programs either in their home or a nursing facility to help control symptoms of CJD at the end of life. Families of individuals with CJD also need emotional support during this time.
Scleroderma is an autoimmune (the body attacking itself) group of diseases from the body making to much collagen (scar tissue). This hardens or tightens the skin and or connective tissues in the human body.
Affects women (80%) more than men (20%). Starts between 30-50 years old. Approximately, 100, 000- 300, 000 cases exist in the United States. No cure exists.
Causes
genetics, exposure to virus or bacteria infections, silica, and certain medications, and abnormal immune system
Diagnosis
Scleroderma is diagnosed by symptoms and ruling out other causes. This can be a long and frustrating process, estimated to be about 3 years.
Rhuematologists are specialized doctors that are often involved in the diagnosis and treatment of scleroderma. They or other doctors caring for you may order blood work, computer tomography (CT) and Xrays to rule out other diseases. Ultrasound and magnetic resolution imagery (MRI) may be used to look at tissue deep within your body.
Image from Medscape
Signs and Symptoms
skin The skin becomes hardened and tight. It may look shiny. Movement may become difficult because of the tight, hard skin.
Image by Merck Manuals
Raynaud’s Phenomenon Small blood vessels in hands and feet contract (become smaller) in cold temperatures or because of emotional distress. Toes and fingers may feel cold to touch, become numb, painful and even have a blue color. Raynaud’s phenomenon may happen when a person does not have scleroderma.
digestive symptoms Symptoms vary based on which tissues are affected but can include: difficulty swallowing, heart burn, cramping, bloating, constipation, and difficulty absorbing nutrients.
heart Scarring on the heart can create irregular and deadly heart rhythms. High blood pressure (hypertension) . Swelling in legs and shortness of breath are common in congestive heart failure (CHF).
lungs Scaring on the lungs can cause difficulty breathing and dangerously low oxygen levels in the body. This may be called pulmonary hypertension by your doctor.
kidneys Scarring in these organs can lead to high blood pressure and difficulty eliminating toxins in the form of urine.
mouth Tightening of skin on the face can lead to difficulty brushing teeth or having them cleaned professionally. Decreased amounts of saliva (spit) are produced. This increases the risk of cavities.
sex organs Men may experience difficulty getting or maintaining an erection (getting hard). Women are more likely to decreased vaginal lubrication and narrowing of the vaginal opening.
Treatment
Image by Dreamstime
Treatment of scleroderma is based on symptoms a person is having.
sildenafil (Viagra), tadalafil (Cialis) These medications are know to help men get and maintain erections. They are also used to treat the symptoms of Raynaud’s Phenomenon and pulmonary hypertension.
omeprazole (Prilosec) Proton-pump inhibitors such as Prilosec help reduce heart burn symptoms.
enalapril (Vasotec), lisinopril (Zesteril) ACE inhibitors such as these medications may be used to control high blood pressure, congestive heart failure, and damage to the kidneys.
Immune suppressants and immune globulin are medications being used to treat muscle pain and weakness